Lowering bill rates.
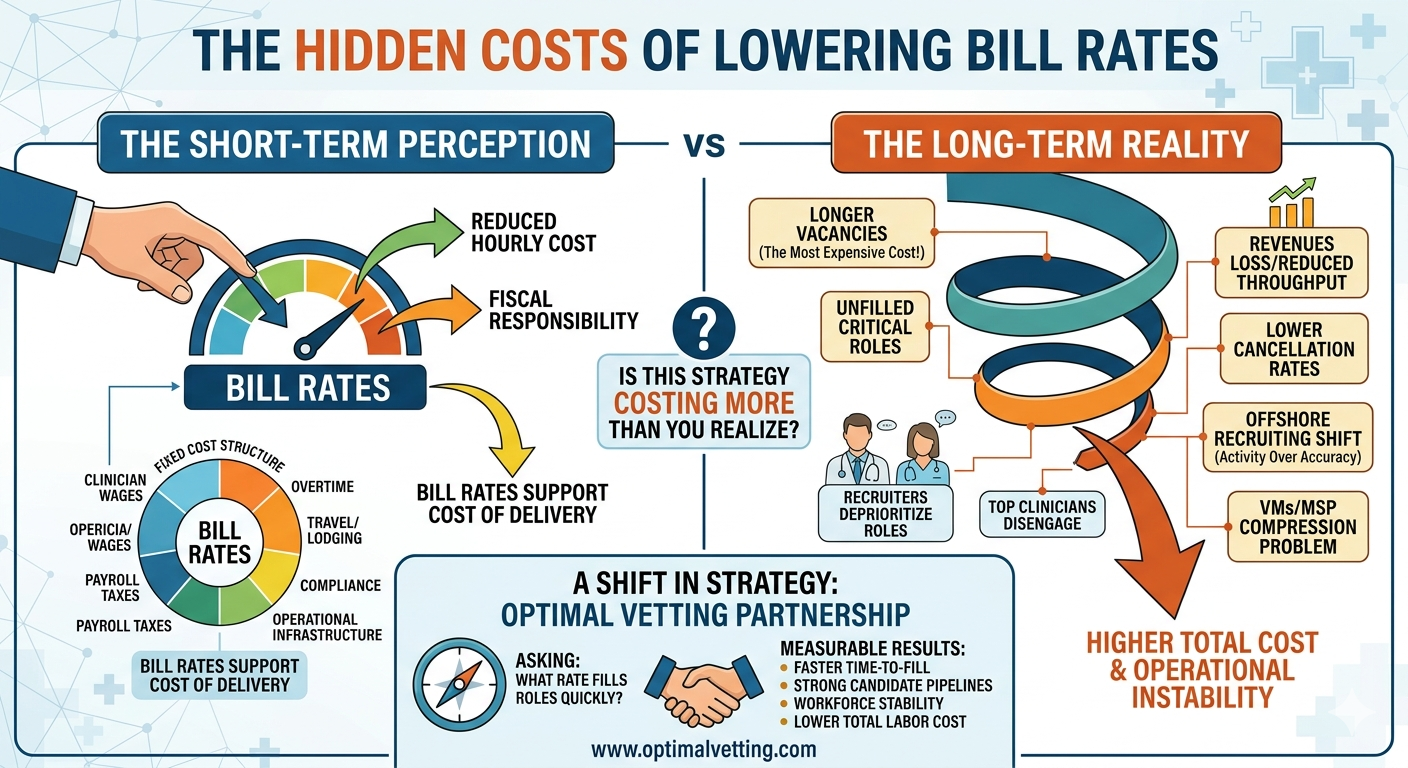
On the surface, reducing hourly rates appears fiscally responsible. In practice, it often leads to higher costs, longer vacancies, and operational instability. The issue isn’t the intent to control cost—it’s the way cost is being measured.
Most organizations evaluate staffing decisions based on hourly rate alone. Yet total labor cost is shaped by a very different set of variables:
- How long critical roles remain unfilled
- How quickly qualified candidates are submitted
- Whether clinicians complete their assignments
- The level of overtime absorbed by internal teams
When bill rates fall below market, these variables deteriorate almost immediately:
- Recruiters deprioritize the role
- Top-performing clinicians disengage
- Submission volume drops—or unqualified submissions increase
- Time-to-fill expands
At that point, the organization is no longer competing for talent—it’s being bypassed by it.
Bill Rates Don’t Reflect Agency Margin-They Reflect Cost of Delivery
A common misconception is that bill rates primarily represent agency profit. In reality, they support a fixed cost structure that includes:
- Clinician wages
- Overtime
- Travel and lodging
- Payroll taxes
- Compliance
- Operational infrastructure
Travel and housing costs, in particular, are not discretionary. They are typically aligned with federal per diem guidelines and are required to deploy clinicians. These are not profit centers.
When bill rates are pushed down, the only adjustable variable becomes clinician pay. And when compensation becomes uncompetitive, access to talent declines.
The California Effect: When Overtime Isn’t Optional
This dynamic becomes even more pronounced in states like California, where overtime is triggered after eight hours in a workday. A standard twelve-hour shift includes four hours at time-and-a-half.
If overtime is not reimbursed, it doesn’t disappear—it shifts. Agencies must absorb the cost unless bill rates are structured to account for it. The result is predictable:
- Reduced clinicians pay
- Fewer qualified candidates
- Slower fills
- Lower assignment completion rates
The VMS/MSP Compression Problem
VMS/MSP models offer visibility and standardization, but they also introduce an additional margin layer—often 3% to 7%—that compresses the rate available to the supplying agency.
The agency remains responsible for the full cost of delivery, but with reduced financial flexibility. This leads to:
- Pressure on clinician compensation
- Reduced supplier participation
- Increased difficulty filling roles
The Offshore Recruiting Shift-and Its Hidden Impact
Rate compression has triggered another trend: agencies shifting sourcing and recruiting functions offshore.
While this reduces internal costs for the agency, it often introduces unintended consequences for healthcare organizations. Offshore teams are frequently tasked with high-volume outreach under aggressive productivity expectations. Activity becomes the priority—not accuracy.
What this model often lacks:
- Deep understanding of U.S. healthcare systems
- Nuanced screening for unit-specific experience
- Real-time communication with candidates
- Accountability for long-term placement success
The result is a higher volume of submissions, but not necessarily higher quality.
Healthcare organizations may experience:
- Increased screening burden
- Higher interview-to-offer ratios
- More candidate fall-offs
- Early assignment terminations
Each of these outcomes increases the cost of hiring—not just financially, but operationally.
What appears efficient at the front end often creates inefficiency at the point of care.
Vacancy Is the Most Expensive Cost in Your Organization
An unfilled clinical role drives:
- Overtime
- Burnout
- Reduced patient throughput
- Revenue loss tied to unstaffed capacity
The longer the vacancy persists, the more expensive it becomes.
Leading organizations are shifting their approach. They are no longer asking:
“How do we pay less?”
They are asking:
“What rate allows us to fill this role quickly with the right clinician who will stay?”
This shift produces measurable results:
- Faster time-to-fill
- Stronger candidate pipelines
- Higher assignment completion rates
- Improved workforce stability
- Lower total labor cost
The most expensive position in your hospital is not the one you fill at a higher rate-it’s the one that remains unfilled.
If Your Costs Are Rising Despite Lower Rates, the Issue May Not Be Staffing-It May Be Strategy
Optimal Vetting partners with healthcare organizations to align staffing strategy with financial and operational outcomes. We are not a staffing vendor – we help hospitals and health systems:
- Structure competitive, market-aligned bill rates
- Navigate VMS/MSP environments effectively
- Ensure a disciplined, quality-driven recruiting approach—without sacrificing speed
To discuss your current strategy or request a workforce cost analysis, visit www.optimalvetting.com.
The question is not whether you are spending on staffing. It is whether your current approach is costing you more than you realize.